Yesterday, while most of LA was trying to escape a fire that had broken out along the 405 near the Getty Museum my wife, Jodie and I raced towards it. I had an appointment with Dr. Stuart Holden, a urological oncologist at UCLA that had been recommended to me by a family friend.
I can best describe the UCLA Medicine complex as what would happen if a hospital building devoured several other hospital buildings and then plopped itself down in the middle of a bustling downtown. The size was bewildering! While checking in at Urology Jodie noticed that all of the doctors’ cards were arranged on a turnstile like the ones grocery stores use to display gift cards. We counted over 30 before finding and pocketing Dr. Holdens.
It’s amazing how different doctors can have such dramatically different opinions on treatment.
Last week I talked to Dr. Carrie Costantini, an oncologist at Scripps. She gave me two options, either remove my prostate, or bombard it with radiation. Dr. Holden told me that performing surgery was premature without first determining if the cancer had spread. He said that the treatment varies considerably depending on whether or not the cancer is contained within the prostate or has spread elsewhere. Furthermore, performing surgery or treatment before getting a full picture might make me ineligible for clinical trials.
Dr. Holden told me that out of the 60 urologists in his office that none of them would preemptively operate without running additional tests.
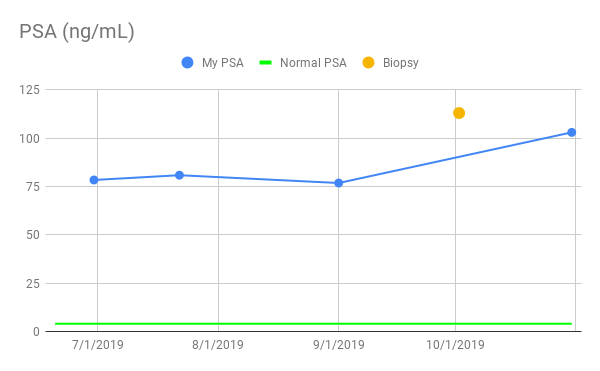
These tests include a bleeding edge scan called a Ga-PSMA PET CT Scan. What a mouthful, right? In my last post I wrote about the Prostate-specific antigen ( PSA ) test for helping to detect prostate cancer. To clarify, PSA is a protein produced by the prostate. When the prostate is inflamed it produces more of it. Thus, it is commonly used as an indicator of cancer. As it turns out once prostate cancer has metastasized the PSA protein is not as accurate, particularly with aggressive cancer such as yours truly has. The Prostate-specific membrane antigen ( PSMA ) is another protein that’s prevalent in metastasized prostate cancer cells. This new PSMA scan can pinpoint exactly where prostate cancer has metastasized so that targeted drugs can be delivered. Or, at least that’s what Dr. Holden is trying to sell me on. The truth is? I believe him. The downside is that the test costs just shy of $3000, is not ( yet ) FDA approved, and I’ll have to drive UCLA to get it done. Hopefully the fires will have been extinguished by then.
Dr. Holden also wanted me to get a genetic screening done as he suspects my cancer is likely well, genetic. Whereas Scripps told me there was a 4 month lead time, Dr. Holden directed me to a company called Color Genomics. For $249 and some of your spit Color Genomics will determine if you have any known cancer genes including BRCA-1 and BRCA-2. BRCA stands for “BReast CAncer susceptibility gene”. Dr. Holden told me that my cancer treatment could vary based upon the findings produced by the genetic screening. Having the genetic screening performed will also help determine if my daughters might be at risk of cancer someday as well.
Lastly, Dr. Holden was perplexed why my initial CT Scan did not include my entire body. He told me that given my high PSA ( 78+ ) and Gleason ( 8-10 ) scores that it would be highly unlikely that the cancer would not have already metastasized. He told me that this warranted a CT Scan of my entire body – not just my groin area. He said that the CT Scan that I received was an impartial picture of the problem. Dr. Holden was just as perplexed why my prostate biopsy wasn’t guided by Magnetic Resonance Imaging ( MRI ). A urologist has the option of using an MRI machine to target specific regions of the prostate during a biopsy. My urologist removed 12 samples, or cores randomly from my prostate. In his defense however, he struck “gold” everywhere he dug.
Then Dr. Holden gave me yet another Digital Rectal Exam.
I’m beginning to realize that Prostate Exams are to a urologist as handshakes are to everyone else.
It’s just their way of saying, “Hi. Nice to meet you.” Fortunately, Dr. Holden admitted to having small hands before niceties were exchanged.
So what’s next? This Friday I have another second ( third? ) opinion with a Dr. Tyler Stewart a urological oncologist at UCSD’s Moores Cancer Society. After that I’ll have more than enough information to make an educated decision on what to do next.
Not for the last time I am incredibly grateful for the outpouring of support from everyone as I work through all of this. I can’t thank you enough. I’m beginning to realize that cancer is a full-time job but at the same time it’s important not to lose sight of what is important. I love you all. Take care. Eat Healthy. Stay Healthy.
Take care. Stay healthy. Live life.
-Scott
Previous : Prostate Cancer
Next : Building My Team

#prostatecancer #cancer #prostatitis #psa #prostate #urology #oncology #drawnandcoded #iwillbeatthis